Dental surgical instruments are the foundation of every successful oral surgery procedure. Whether you are a dental student preparing for board exams, a dental professional building a surgical kit, or a patient wanting to understand what happens during treatment, knowing the correct dental surgical instruments names is essential.
This expert-reviewed guide covers 30+ dental surgical instruments with their names, specific uses, types, and clinical applications — organized by category and procedure. It follows EEAT (Experience, Expertise, Authoritativeness, Trustworthiness) standards used in professional dental education.
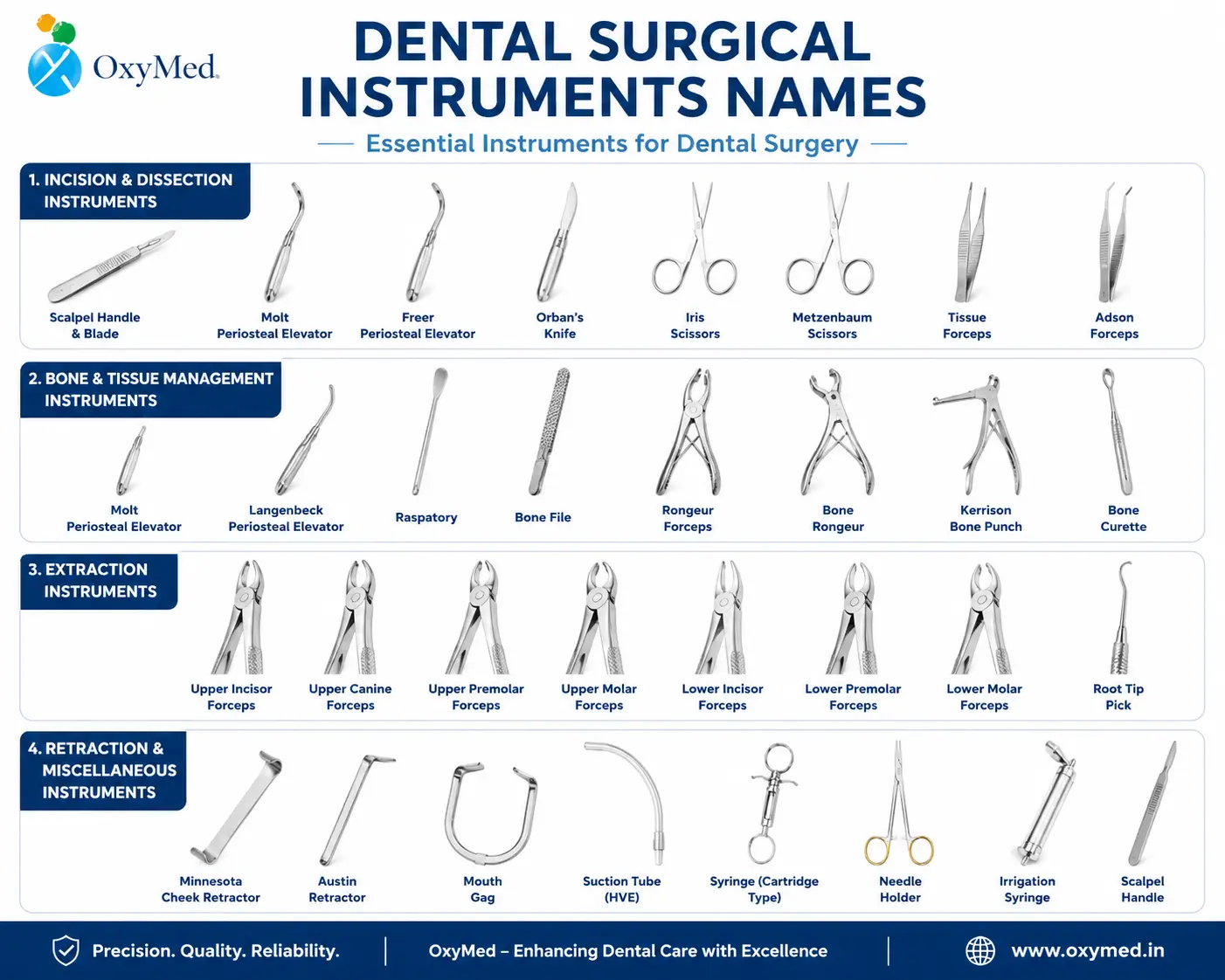
Dental surgical instruments are specialized precision tools used by oral surgeons, general dentists, and dental specialists to perform extractions, incisions, suturing, bone reshaping, implant placement, and tissue management. Most are manufactured from German-grade or surgical-grade stainless steel for durability, corrosion resistance, and repeated autoclave sterilization.
Dental instruments are broadly grouped into five functional categories:
| Category | Primary Function | Examples |
|---|---|---|
| Diagnostic | Examination and detection | Mirror, explorer, periodontal probe |
| Surgical | Extractions and oral surgery | Forceps, elevators, scalpels, rongeurs |
| Restorative | Cavity fillings and repairs | Amalgam carrier, condenser, carver |
| Prophylaxis | Cleaning and scaling | Scalers, curettes, prophy cups |
| Endodontic | Root canal treatment | K-files, broaches, spreaders |
Primary use: Grasp and remove teeth from the alveolar socket during extraction procedures.
Extraction forceps are among the most critical dental surgical instruments. They are available in multiple designs matched to specific teeth and jaw positions. The beaks of forceps are shaped to fit the anatomy of each tooth type, providing a secure grip while minimizing bone and soft tissue trauma.
Types of Extraction Forceps and Their Uses:
| Forceps Name | Number | Specific Use |
|---|---|---|
| Universal Forceps | — | General-purpose tooth extraction |
| Upper Anterior Forceps | 150 | Maxillary centrals, laterals, cuspids |
| Lower Anterior Forceps | 151 | Mandibular anterior teeth and premolars |
| Upper Molar Forceps (Left) | 88L | Left maxillary molars |
| Upper Molar Forceps (Right) | 88R | Right maxillary molars |
| Lower Molar Forceps | 17 | Mandibular molars |
| Upper Root Tip Forceps | 65 | Fragile root tips in upper arch |
| Pediatric Forceps | Various | Deciduous (baby) tooth extraction |
Clinical tip: Always match forceps to the specific tooth being extracted. Using the wrong forceps increases the risk of root fracture and post-operative complications.
Primary use: Loosen the periodontal ligament and separate the tooth from its bony socket before or during extraction.
Dental elevators work by applying controlled lever force between the tooth root and surrounding alveolar bone. They minimize the force required for forceps extraction, reducing trauma and improving patient recovery. A sharp blade and ergonomic handle are key quality indicators.
Types of Dental Elevators:
| Elevator Name | Shape | Best Use |
|---|---|---|
| Straight Elevator (301) | Straight blade | General single-rooted tooth extraction |
| Cryer Elevator (East/West) | Paired, triangular | Difficult mandibular molar extractions |
| Potts Elevator | Angled | Loosen tooth or root from socket |
| Crane Elevator | Right-angle pick | Luxate and elevate impacted roots |
| Apical Elevator | Thin, curved | Remove apical root fragments |
| Anglevator | Angled hybrid | Complex extractions with limited access |
| Luxator | Ultra-thin blade | Minimal-trauma extraction; severs periodontal ligament |
| Coupland Elevator | Three-piece set | Socket expansion and dilation |
Primary use: Lift and retract the gingival and periosteal tissue away from the bone to expose the surgical field during incisional (flap) extractions, implant placement, and bone surgeries.
The West Periosteal Elevator is the most commonly used type. It is double-ended, with one flat and one pointed end. A sharp working end is essential — a dull periosteal elevator shreds soft tissue flaps rather than lifting them cleanly.
Common types: West Elevator, Molt No. 9, Freer Elevator
Primary use: Make precise, clean incisions through gingival and mucosal tissue to create surgical flaps for tooth extractions, implant surgery, biopsies, and periodontal procedures.
Scalpels consist of a reusable handle and a disposable sterile blade. The blade is replaced between surgeries to maintain cutting precision and prevent cross-contamination.
Common scalpel handles and blades:
| Handle / Blade | Use |
|---|---|
| Handle No. 3 | Standard handle for most dental procedures |
| Blade No. 15 | Most common dental blade; curved for precise intraoral cuts |
| Blade No. 12 | Sickle-shaped; posterior access and releasing incisions |
| Blade No. 11 | Pointed; stab incisions and abscess drainage |
Primary use: Cut soft tissue, excise diseased tissue, and remove sutures during and after oral surgical procedures.
| Scissors Name | Key Feature | Use |
|---|---|---|
| Kelly Scissors | Straight or curved blades | Cutting excess or diseased soft tissue |
| Dean Scissors | Angled blades | Tissue excision; improved posterior access |
| Spencer Suture Scissors | Small, fine blades | Cutting sutures intraoperatively and during removal |
| Iris Scissors | Very fine tips | Delicate tissue dissection |
| Metzenbaum Scissors | Long, slender blades | Blunt dissection of deep tissues |
Primary use: Securely grip and pass a suture needle through tissue to close surgical wounds after oral surgery, extractions, and implant procedures.
A needle holder features a locking ratchet mechanism that holds the needle firmly at the correct angle. The jaw design prevents needle rotation during suturing. Proper needle placement in the holder — at the junction of the middle and distal thirds — ensures control and prevents needle bending.
Common types: Crile-Wood Needle Holder, Mayo-Hegar Needle Holder, Castroviejo Needle Holder (for fine sutures)
Primary use: Clamp blood vessels or grasp tissue to control bleeding during oral surgical procedures.
Hemostats have a locking ratchet mechanism similar to needle holders. They are used to compress vessels, hold tissue away from the surgical field, and assist with suture management.
Types: Mosquito Hemostats (small vessels), Kelly Hemostats (medium vessels), Crile Hemostats (larger tissues)
Primary use: Grasp, hold, and manipulate soft tissue during incisions, suturing, and tissue excision procedures.
| Type | Description |
|---|---|
| Adson Forceps | Fine, serrated tips; precise tissue handling |
| College (Cotton) Forceps | Transfer materials; hold gauze or cotton rolls |
| Allis Forceps | Locked grip for firmer tissue holding |
| Russian Forceps | Broad, round tips; atraumatic tissue holding |
Primary use: Trim, contour, and remove sharp or irregular bone edges following tooth extraction or during bone surgery.
Rongeurs are spring-action cutting instruments with sharp cup-shaped jaws that bite away bone. They are essential after extraction of impacted teeth where bone edges need smoothing before wound closure.
Types:
Primary use: Cut and reshape larger sections of bone during advanced oral surgical procedures, including complex impactions and alveoloplasty (bone reshaping before denture placement).
These are heavier instruments than rongeurs and are used when significant bone reduction is required.
Primary use: Split or section bone and teeth during surgical extractions of impacted teeth, particularly mandibular third molars (wisdom teeth).
Bone chisels are driven with a surgical mallet. The beveled blade cuts through bone cleanly with minimal heat generation, unlike rotary instruments.
Types: Straight Chisel, Bin-Angle Chisel, Wedge Chisel
Primary use: Smooth and refine bone surfaces after rongeurs have removed the bulk of irregular bone, creating a smooth foundation for wound healing and denture fit.
Bone files work in a push-pull motion and are available in single-cut and cross-cut patterns.
Primary use: Scrape, remove, and clean soft tissue debris, granulation tissue, and infection from bony sockets after tooth extraction.
| Curette Name | Description |
|---|---|
| Lucas Bone Curette | Angled, double-ended, spoon-shaped; scrapes socket walls |
| Molt Bone Curette | Removes tissue and debris from bony sockets |
Primary use: Retrieve small, fractured, or loose root fragments remaining in the alveolar socket after tooth extraction.
Root tip picks have extremely fine, angled tips designed to reach apical areas of the socket where standard forceps cannot access. Leaving root fragments in the socket risks infection and delayed healing.
Primary use: Hold the cheek, tongue, and soft tissues away from the surgical field to improve visibility and protect tissues during procedures.
| Retractor Name | Use |
|---|---|
| Minnesota Cheek Retractor | Retract cheek and tongue simultaneously; most widely used |
| Weider Tongue Retractor | Keep tongue depressed during lower arch surgery |
| Austin Retractor | Hold tissue flaps and cheek during implant surgery |
| Seibert Retractor | Posterior tissue retraction |
Primary use: Hold the patient's mouth open during procedures, particularly under sedation or general anesthesia, or for patients with limited mouth opening.
| Instrument | Use |
|---|---|
| Molt Mouth Gag | Spring-action; holds mouth open; adjustable |
| Mouth Prop (Bite Block) | Simple rubber or silicone prop; placed between teeth |
Primary use: Flush the surgical site, socket, or wound with sterile saline or chlorhexidine solution to remove debris, blood clots, and bacteria during and after surgery.
A surgical irrigation syringe with a curved or blunt tip allows targeted flushing of deep sockets and inaccessible areas without damaging surrounding tissue.
Primary use: Deliver local anesthetic solution to the target nerve site before any surgical procedure.
The aspirating syringe allows the clinician to pull back the plunger before injecting to confirm the needle is not inside a blood vessel. This is a critical safety step. Most are breech-loading stainless steel syringes fitted with a sealed anesthetic cartridge.
Primary use: Remove blood, saliva, irrigation fluid, and debris from the oral cavity to maintain a clear surgical field throughout the procedure.
| Type | Use |
|---|---|
| Yankauer Suction | Rigid wide-bore tip; general oral suctioning |
| Frazier Suction | Thin, angled tip; precise suctioning in small areas |
| Surgical Aspirator Tip | Fine tip for socket and flap surgery irrigation |
Primary use: Stabilize and immobilize the jaw following mandibular or maxillary fractures; maintain the natural bite relationship during healing.
Arch bars are wired to the teeth along the arch and used in maxillofacial trauma management and orthognathic surgery.
These instruments are used before surgery to examine, measure, and assess the patient's oral condition.
Use: Visualize the oral cavity including tooth surfaces, gingival tissue, palate, tongue, and cheeks. Reflects indirect light into difficult areas and retracts soft tissues.
Types: Front-surface mirror (distortion-free), rhodium-coated mirror, disposable plastic mirror
Use: Detect dental caries (cavities), calculus deposits, surface irregularities, and defective restorations by tactile examination of tooth surfaces.
| Explorer Type | Number | Best For |
|---|---|---|
| Shepherd's Hook | No. 23 | General caries detection, gingival margins |
| Back Action (Pigtail) | No. 17 | Proximal tooth surfaces |
| Right-Angle Explorer | No. 2 | Subgingival calculus; posterior areas |
Use: Measure the depth of periodontal pockets around each tooth in millimeters to assess gum disease severity, bone loss, and tissue health before surgical intervention.
Calibrated in millimeter markings (1–10 mm). Pocket depths over 4 mm generally indicate periodontal disease requiring treatment.
| Instrument | Description | Use |
|---|---|---|
| Amalgam Carrier | Hollow barrel with plunger | Carry and deliver amalgam filling material into the prepared cavity |
| Condenser (Plugger) | Flat or serrated working end | Pack and condense filling material into cavity |
| Cleoid-Discoid Carver | Double-ended; claw and disc shaped | Carve occlusal anatomy into amalgam before setting |
| Burnisher | Smooth, rounded end | Smooth and polish amalgam restorations |
| Mixing Spatula | Flexible blade | Mix dental cements, composites, and impression materials |
| Matrix Band and Retainer | Thin metal band with clamp | Restore wall of tooth during filling procedures |
| Instrument | Use |
|---|---|
| Hand Scaler (Sickle Scaler) | Remove supragingival calculus and plaque from tooth surfaces |
| Ultrasonic Scaler | Remove calculus using high-frequency vibrations plus water irrigation; faster than hand scaling |
| Periodontal Curette (Gracey Curette) | Root planing; clean below gum line; remove subgingival calculus |
| Prophy Cup / Prophy Brush | Polish tooth surfaces with prophylaxis paste |
| Air Polisher | Remove stains and plaque using pressurized air and sodium bicarbonate powder |
| Instrument | Use |
|---|---|
| High-Speed Handpiece | Cut enamel and dentin; tooth preparation; bone cutting during surgery |
| Low-Speed Handpiece | Polish, shape, and finish restorations; slow-speed surgical drilling |
| Surgical Handpiece | Bone cutting during implant surgery, wisdom tooth removal, and alveoloplasty |
| Round Bur | Caries removal; initial cavity entry |
| Fissure Bur | Cavity preparation and tooth sectioning |
| Surgical Carbide Bur | Cut bone and tooth structure during oral surgery |
| Diamond Bur | Cutting, shaping, and finishing enamel and porcelain |
| Instrument | Use |
|---|---|
| Barbed Broach | Remove pulp tissue from root canal; thin, flexible wire with barbed edges |
| K-File | Clean, shape, and enlarge root canal walls |
| H-File (Hedstrom) | Aggressive cutting action; canal shaping |
| Endodontic Spreader | Compact gutta-percha filling material laterally inside canals |
| Endodontic Plugger | Vertically compact root canal filling material |
| Endodontic Explorer | Locate root canal orifices on the pulp chamber floor |
| Rubber Dam Clamp and Forceps | Isolate the tooth for moisture-free root canal treatment |
Dental professionals typically work from procedure-specific instrument trays. Here are the standard instrument sets:
All basic extraction instruments plus:
All surgical extraction instruments plus:
Here is a master reference list of 35+ essential dental surgical instruments:
The quality of a dental surgical instrument directly affects procedure outcomes. Key quality indicators:
Material: Surgical-grade or German stainless steel resists corrosion, maintains sharpness through repeated sterilization, and does not flex under pressure.
Finish: Satin or matte finishes reduce glare under operating lights. Mirror-polished finishes are used on diagnostic instruments.
Balance and Weight: Ergonomically balanced instruments reduce operator fatigue during long surgical procedures.
Blade Sharpness: Scalpels, elevators, and curettes must maintain a fine cutting edge. Dull edges require more force and cause greater tissue damage.
Proper sterilization prevents cross-contamination, protects patient safety, and extends instrument lifespan. The standard sterilization protocol in dental practice follows FDA and CDC guidelines:
Step 1 — Immediate post-use cleaning: Rinse instruments under running water immediately after use to prevent blood and tissue from drying.
Step 2 — Ultrasonic cleaning: Place instruments in an ultrasonic cleaning unit for 5–10 minutes. Ultrasonic vibrations remove debris from instrument joints, serrations, and grooves that manual scrubbing cannot reach.
Step 3 — Rinse and dry: Rinse with distilled water and dry thoroughly before packaging.
Step 4 — Packaging: Seal instruments in sterilization pouches with chemical indicator strips before autoclaving.
Step 5 — Autoclave sterilization: Steam autoclave at 134°C (273°F) for 3–4 minutes (pre-vacuum cycle) or 121°C (250°F) for 15–30 minutes (gravity cycle). This kills all bacteria, viruses, spores, and fungi.
Step 6 — Storage: Store sealed, sterilized pouches in a clean, dry, dust-free area. Do not open pouches until the instrument is needed.
Step 7 — Inspection and replacement: Inspect instruments before each use for cracks, broken tips, locked hinges, or dull blades. Replace any instrument that does not meet clinical standards.
For Dental Professionals:
Correct instrument identification prevents wrong-instrument errors during surgery, improves team communication between dentist and dental nurse, and ensures the right tool is selected for each step of the procedure.
For Dental Students:
Instrument identification is tested in INBDE, NBDE, and ADAT board examinations. Clinical competence in instrument recognition is assessed during supervised clinical rotations.
For Dental Assistants and Nurses:
Rapid, accurate instrument passing during surgery depends entirely on knowing each instrument by name and function. Incorrect instrument passing slows procedures and increases patient discomfort.
For Patients:
Understanding the instruments used in dental procedures reduces pre-treatment anxiety, enables informed consent, and improves patient communication with their dental care provider.
Mastering dental surgical instruments names is foundational knowledge for anyone in the dental field. From extraction forceps and dental elevators to scalpels, bone rongeurs, needle holders, and root tip picks, each instrument serves a specific, irreplaceable function in oral surgery.
This guide has covered 40+ instruments across all major dental surgical categories — organized by instrument type, procedure tray, and clinical application — giving you a complete, EEAT-compliant reference for study, clinical practice, and exam preparation.
Use this guide as your go-to reference whether you are setting up a dental surgical kit, studying for board exams, or simply want to understand the tools behind modern oral surgery.
The most frequently used dental surgical instruments are extraction forceps, dental elevators, periosteal elevators, scalpels with blade No. 15, surgical scissors, needle holders, hemostatic forceps, bone curettes, and irrigation syringes. Every oral surgery procedure requires at minimum an extraction forceps, elevator, and suction aspirator.
Dental elevators loosen the periodontal ligament and separate the tooth from the socket before extraction using leverage. Extraction forceps then grasp the loosened tooth and remove it from the socket. Elevators prepare the tooth; forceps complete the extraction.
Q3: How many types of dental extraction forceps are there?
There are over 20 types of extraction forceps matched to specific teeth and jaw positions. The most common include Forceps No. 150 and 151 (anterior teeth), No. 88L and 88R (upper molars), No. 17 (lower molars), No. 65 (root tips), and pediatric forceps sets for primary teeth.
The Root Tip Pick (also called apical pick or root tip forceps) is specifically designed to retrieve fractured or retained root fragments from the alveolar socket after extraction.
A luxator is a thin, sharp-bladed elevator designed to sever the periodontal ligament and expand the socket wall before extraction. It causes minimal trauma and is especially useful in atraumatic extraction techniques for patients requiring implants.
A periosteal elevator lifts the gingival and periosteal tissue away from underlying bone to create surgical flaps during complex extractions, implant surgery, and bone procedures. The Molt No. 9 and West periosteal elevator are the most commonly used types.
Spencer Suture Scissors are specifically designed for cutting sutures both intraoperatively and during postoperative suture removal. Their fine, short blades allow precise suture cutting close to the tissue without disturbing wound closure.
Dental surgical instruments should be cleaned immediately after use, ultrasonically cleaned to remove debris, sealed in sterilization pouches, and autoclaved at 134°C for 3–4 minutes or 121°C for 15–30 minutes following FDA and CDC sterilization guidelines.
Bone rongeurs are used to trim and contour irregular or sharp bone edges after tooth extraction, particularly after removing impacted wisdom teeth. They smooth the alveolar crest before wound closure and help prepare the ridge for future dentures or implants.
Surgical removal of impacted wisdom teeth typically requires a local anesthetic syringe, scalpel with blade No. 15, periosteal elevator, cheek retractor, surgical handpiece with carbide burs, bone rongeurs, bone file, extraction forceps, elevators (Cryer, straight), irrigation syringe, needle holder, suture scissors, and suture material.
Also Follow Us: Facebook, Instagram
©Copyright 2026 All Rights Reserved.

